Through the Suicide & Crisis Lifeline and other efforts, McKinsey Health Institute is helping develop a community-based approach to crisis care across the United States.
Editors’ Note: If you’re experiencing a suicide or mental health crisis, please contact a crisis help line in your country (988 in the United States). For more information about World Suicide Prevention Day, please refer to these resources from the World Health Organization and the US Substance Abuse and Mental Health Services Administration. There are many excellent actions employers can take, including examples from: Mental Health First Aid, MQ Mental Health, and the International Association for Suicide Prevention.
On a winter morning in late 2019, Kana Enomoto sat in an emergency room outside of Washington, D.C., with her teenage daughter, Reina, feeling helpless and scared.
Three days earlier, Reina, 15 at the time, had acted on suicidal thoughts, and Kana spent nearly every hour since searching for mental health crisis resources for adolescents. Everyone told her the same thing: take her to the ER. Kana, who is now the director of brain health at the McKinsey Health Institute, is also a 25-year veteran in the behavioral health arena and knew the ER wouldn’t help her daughter—but there was no other option.
The doctor recommended inpatient care, but no beds were available, so for three and a half days, Reina was confined to a glass-walled room under bright lights and constant surveillance, isolated from everyone except her mom, who slept in the hospital chair next to her as they waited for a bed to open up in the adolescent psych unit.
“Sitting in an emergency room for days at a time, not being able to get the help your kid needs is devastating,” Kana says. “I had advocated for evidence-based mental health services throughout my career, yet couldn’t find them for my own child.”
A growing behavioral health crisis
Kana and Reina’s experience isn’t uncommon. In the United States, crises related to behavioral health, a term that refers to both mental and substance use disorders, have been on the rise for more than two decades—particularly among youth. Between 2009 and 2020, the United States saw a 30 percent increase in the national age-adjusted suicide rate. By winter of 2021, the weekly rate of ER visits by adolescents who attempted suicide was 39 percent higher than pre-pandemic levels, and the average rate for adolescent girls had increased 50 percent over the previous year.
-
39% more ER visits a week by teens attempting suicide than pre-pandemic level
-
30% higher suicide rate in the US between 2009 and 2020
-
39M people per year could benefit from a crisis hotline
Despite these alarming numbers, community crisis-care resources remain limited. According to the 988 Suicide & Crisis Lifeline center, roughly 39 million Americans aged 12 and older could benefit from having access to a service for vulnerable people dealing with suicide, mental health, or substance use issues. Limited crisis services mean law enforcement, emergency medical services (EMS), and ERs end up responding to most behavioral health crises, regardless of whether the individual is a threat to public safety or in need of emergency care.
“What we’re doing now is services that are high cost and low efficacy,” says Kana. “It’s the wrong recipe.”
Dr. John Palmieri is a senior medical advisor and the acting director of the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Behavioral Health Crisis Team, which includes the 988 Lifeline. He spent the early part of his clinical career working in emergency psychiatric departments and witnessed firsthand the misdirection of care and resources for those in behavioral health crisis.
“You see the downstream effects of where the system fails in so many ways when you’re in those settings day after day,” he says. “How are we looking upstream to prevent these crisis situations from happening in the first place or recurring?”
A hotline to help those in need
The National Suicide Hotline Designation Act, passed in 2020, made “988” the official nationwide three-digit behavioral health crisis number as of July 2022. This meant that, for the first time, those experiencing a behavioral health crisis anywhere in the country would only have to remember three digits to find the appropriate help.
The National Suicide Prevention Lifeline first launched in 2005 as a ten-digit number. At the time, Kana was working for the Center for Mental Health Services at SAMHSA, which oversaw the number’s rollout. Over the years, she watched the Lifeline evolve, expanding to include options for Spanish language, veterans’ crises, and disaster distress help lines. “I’ve been along for the journey of the growth of the Lifeline and saw advocacy from the field trying to advance a three-digit calling number,” she says.
In the first week after 988 launched on July 16, 2022, the total call volume increased by 45 percent and Lifeline counselors answered 23,000 more calls, texts, and chats than the previous week.
The new easy-to-remember number, while hugely promising, raises at least one potential challenge. Call volume—rising over the years—has already begun skyrocketing since the new number launched. In the first week after 988 launched on July 16, 2022, the total call volume increased by 45 percent and Lifeline counselors answered 23,000 more calls, texts, and chats than the previous week.
To help localities and stakeholders across the country prepare for this surge, the McKinsey Health Institute (MHI), the firm’s not-for-profit entity that focuses on addressing public health challenges, has been involved in a range of nationwide efforts. This includes helping ensure states, contact centers, first responders, and community behavioral health providers know exactly what they need to meet demand—be it new strategies, workforce training, data infrastructure upgrades, or other support.
Defining effective crisis care
In December 2020, MHI came together with a group of national behavioral health and crisis-care stakeholders for a series of working sessions organized by Vibrant Emotional Health, the not-for-profit administrator of the 988 Suicide & Crisis Lifeline; RI International, a global organization focused on the design and delivery of behavioral health crisis services; and the National Association of State Mental Health Program Directors (NASMHPD). The goal was to help prepare for the launch of 988.
MHI began by listening to 911 managers, mental health and substance-use treatment providers, contact center operators, and first responders to develop a consensus around the critical dimensions of crisis care. MHI gathered input from participating partners on what critical elements of community-based crisis care were necessary for the delivery of the 988 Lifeline.
These conversations helped establish a shared understanding among stakeholders around the priorities of community-based crisis care: ensuring that anyone in crisis has someone to call, someone to help, and a safe place to go, as envisioned in SAMHSA’s National Guidelines for Behavioral Health Crisis Care. Simple as it sounds, this involves developing a continuum of care that includes the 988 crisis line staffed by local workers who can provide information, deescalate crises, and—when in-person support is needed—connect people with nearby services and relevant resources.
Had this kind of response existed in 2019, Kana and her daughter would have had a place to go besides the ER; one that might have provided appropriate care and helped ease already constrained hospital capacity.
Measuring costs and savings involved
What would it take to ensure such crises are handled by trained professionals—including clinicians, peers, and other provider types—across a coordinated continuum of care in every community?
To help answer this question, MHI began working with RI International in 2021 to build the Crisis Resource Need Calculator, a web-based cost calculator that allows local leaders to see a projection of annual behavioral health crisis care costs by county or state. The calculator enables them to understand the cost of providing for every individual in need of local, in-person crisis care based on SAMHSA’s national guidelines. It also considers how many mobile crisis teams states and counties would need, and what resources that would involve to build out to scale.
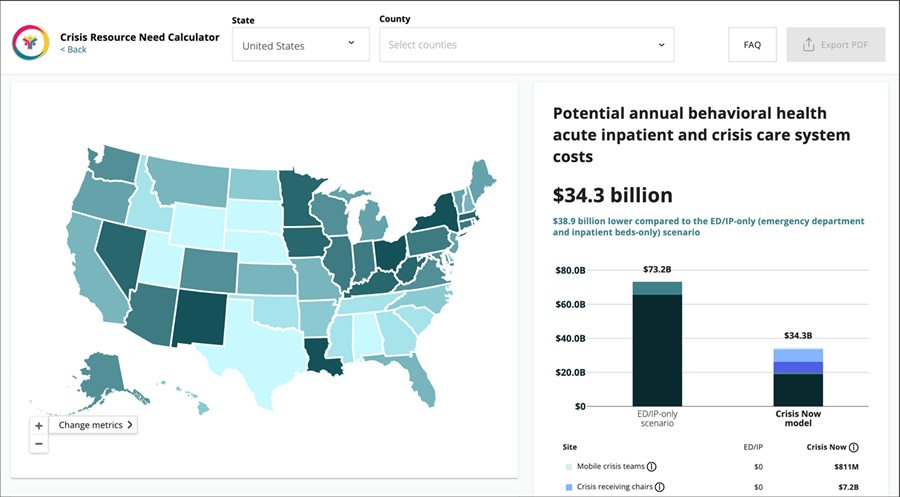
The Crisis Resource Need Calculator also highlights potential healthcare savings available by making this shift in resources. Overall, the calculator estimates that with fully resourced community-based crisis systems in place, the United States could save a total of $34 billion in annual behavioral health costs otherwise spent on ER visits and inpatient beds.
Helping build an action plan
In addition to care costs, MHI also attempted to better assess responder readiness for the transition to 988. To do this, from November 2021 to March 2022, MHI partnered with state, federal, and local entities to develop detailed operational assessment playbooks to help key audiences, including states, tribes and territories, crisis contact operators, 911 centers, and behavioral health providers with understanding how they can prepare for the change.
“The McKinsey team has been the glue that helped put this all together,” says Brian Hepburn, executive director of NASMHPD, which partnered with SAMHSA to prepare for 988’s 2022 rollout. “The effectiveness of the work is dependent on what happens between meetings, and McKinsey filled those gaps with needed data.”
In March 2022, the 988 playbooks were released at a gathering of federal, state, and local stakeholders from across the field. They have since been shared with organizations like the National Council of State Legislators and the National Governors Association to help inform the efforts to scale 988. They’ve also been distributed by partners including the National Emergency Number Association, the National Association for State Alcohol and Drug Abuse Directors, and the National Council for Mental Wellbeing. Each playbook is geared toward a specific crisis-response group, including 911 professionals, Lifeline network contact centers, mental health and substance use disorder treatment providers, states, territories, and tribes.
The playbooks were designed to help state and local leaders understand whether they’re properly staffed, funded, and prepared for 988 response and how to get there. “These playbooks offer stakeholders a self-assessment of their own readiness and links to specific recommendations and tools,” says Brian.
Ensuring equitable care
One of the ongoing challenges these playbooks attempt to tackle is creating equitable crisis care across communities. Ensuring underserved communities have their unique needs taken into consideration is one of the biggest challenges facing the current system, says Shelby Rowe, director of the Suicide Prevention Resource Center.
Shelby, a citizen of the Chickasaw tribe in Oklahoma who has personally experienced suicidal episodes, sits on the board of RI International and advocates for marginalized groups and tribal communities to get access to the full spectrum of crisis care. “If you’re a 15-year-old black trans girl, your experience asking for help in Brooklyn, New York is going to be very different from your experience asking for help in rural Oklahoma,” she says.
Creating a more equitable system requires including diverse voices of those with lived experiences and addressing the underlying challenges and limitations facing specific communities. For example, tribal boundaries don’t always align to state lines, which keeps tribal communities from accessing crisis resource funding; the needs of vulnerable populations like LGBTQ+ youth; the lack of access to crisis response in remote rural communities; the struggles people of color face when attempting to find medical or crisis help, and the list goes on.
“We have an opportunity and an obligation to build a truly equitable crisis response system,” says Shelby.
Creating a sustainable model
Today, crisis response and stabilization services are primarily funded by federal, state, and local governments. Many crisis contact centers are transitioning from trained volunteer workforces to paid specialized staff. Yet an equitable, fully resourced continuum requires sustainable funding and commitment to meet diverse needs across communities.
To support this, MHI and its collaborators, NASMHPD and SAMHSA, are working on several ongoing efforts. This includes examining healthcare claims to better understand how crisis services are paid for, developing a tool to forecast the number of healthcare workers a state or community needs for crisis care, and developing models and strategies to lessen the burden on the crisis workforce. The idea is that state and local governments, payers, and providers can use these resources to better support the current workforce, focus workforce development efforts, and plan for long-term financial sustainability.
“The McKinsey team’s expertise in analytics helped identify some of the root-cause factors driving workforce shortages and what financing models can impact this journey along the crisis treatment system,” says SAMHSA’s John Palmieri.
All of these moving parts come together to steer a broader plan of action for crisis care in the United States. The five-year vision put forth by SAMHSA includes the goal of having 90 percent or more of all 988 calls answered in-state by the end of 2023, up from 71 percent in 2020, and providing 80 percent or more of individuals in the United States with access to mobile crisis response and local services in the next two to five years.
“What’s missing today is widespread, community-based approaches to managing suicidality, mental health crises, and substance use crises both for adults and kids,” says Kana. “Those are the services communities need and getting them actually costs much less and produces better outcomes.”
Including for people like Reina. Since the initial frightening 2019 episode, Kana and her daughter had several others before the family found support through a local county-run organization offering in-home counseling and support to kids and families in need.
Reina has since become an advocate for crisis support for teenagers and started a not for profit in her community to raise awareness for suicide prevention and youth mental health.
“Behavioral health crisis care works and can save lives,” says Kana. “It’s our responsibility across the country to make these services available to people when and where they need them. It’s going take a lot of cross-sector collaboration to transform our nation’s response to behavioral health crises, and MHI is a committed partner along the way.”